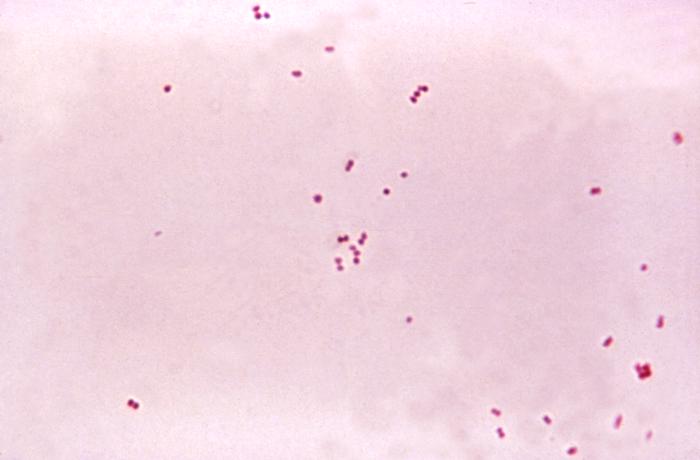
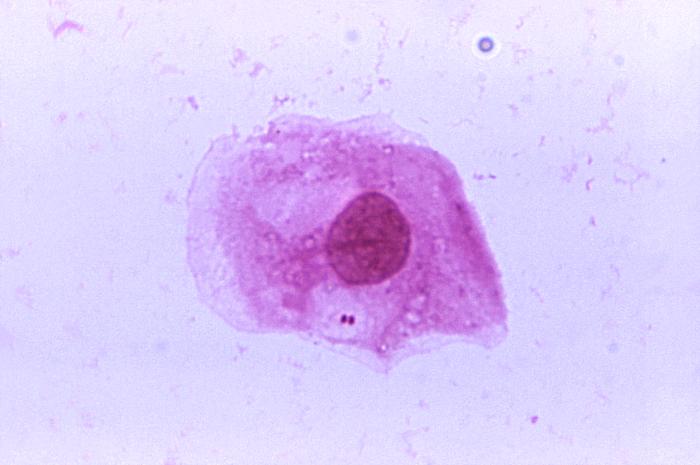
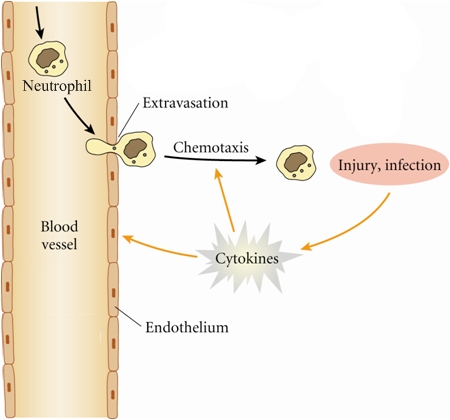
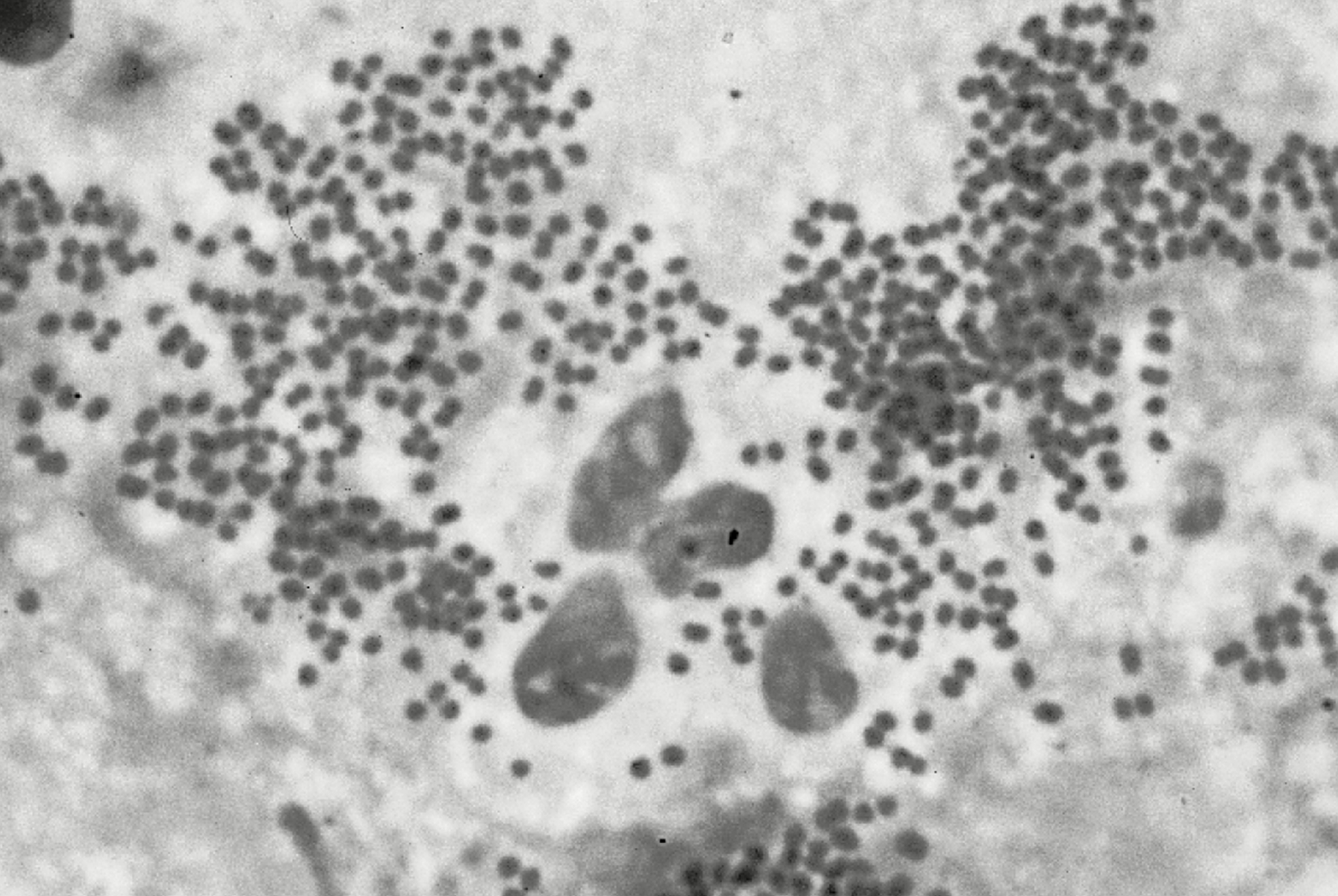
Neisseria meningitidisOverview: Neisseria meningitidis is a Gram-negative diplococcal bacterium responsible for causing meningococcal meningitis (Figure 1). This bacterium is not part of the normal flora, but is found to live in the throat of 5 to 10% of healthy people. It causes the only form of bacterial meningitis known to occur epidemically. Figure 1. This micrograph depicts the presence of aerobic Gram-negative Neisseria meningitidis diplococcal bacteria [1150 X]. Virulence and Pathogenicity: This organism possesses fimbriae (also called pili) on its cell surface and outer membrane components that help it attach to non-ciliated columnar epithelial cells of posterior nasopharynx. This bacteria is also capable of living in the cytoplasm of neutrophils (Figure 2). Figure 2. A photomicrograph of Neisseria meningitidis recovered from the urethra of an asymptomatic male [1125 X]. Since neutrophils use chemotaxis to migrate from blood vessels to inflamed tissues to remove pathogens through phagocytosis and degranulation, N. meningitidis is able to effortlessly infect inflamed tissue, as bacteria travels within the neutrophils throughout the body (Figure 3). Figure 3. The inflammatory response. Black arrows show path of neutrophils from blood to destination at site of injury or infection. N. meningitidis possesses a polysaccharide capsule that makes it easily distinguishable from other Neisseria species. This capsular polysaccharide is an important virulence factor, and there are a variety of different capsules that subdivide the organism into distinct serogroups, namely: A, B, C, H, I, K, L, X, Z, 29E, and W135. Only A, B, C, Y, and W135 are associated with human disease. Other virulence factors include outer membrane proteins called porins (PorA and PorB), that act as B-cell mitogens or activators, and lipooligosaccharide (LOS), a major toxin that acts endotoxically (Singleton et al., 2005). Purified LOS is highly toxic and lethal in mice, and is five to ten times more effective than enteric LPS in causing an inflammatory reaction in rabbits. It leads to suppression of leukotriene B4 synthesis of polymorphonuclear leukocytes, which deprive leukocytes of a chemokinetic and chemotactic factor. In addition, LOS can mutate amino acid residues that can alter interactions with antibodies, allowing it to escape previous immune responses. The LOS is highly sensitive to temperature, so any temperature above or below 37°C will induce dissemination of the LOS, leading to autolysis. Mechanism of Cellular Invasion: Like most bacterial intracellular pathogens, N. meningitidis exploits host cell signaling pathways to promote its uptake by host cells. N. meningitidis does not have a so-called type III secretion system nor a type IV secretion system. The signaling leading to bacterial internalization is induced by the type IV pili (fimbriae), which are the main means of meningococcal adhesion onto host cells. The signaling induced following type IV pilus-mediated adhesion is responsible for the formation of microvilli-like structures at the site of the bacterial-cell interaction. These microvilli trigger the internalization of the bacteria into host cells. A major consequence of these signaling events is a reorganization of the actin cytoskeleton, which leads to the formation of membrane protrusions, engulfing bacterial pathogens into intracellular vacuoles. Efficient internalization of N. meningitidis also requires the activation of an alternative signaling pathway coupled with the activation of the tyrosine kinase receptor ErbB2. Infection and Disease: N. meningitidis can infect susceptible human hosts and can lead to acute bacterial meningitis, also known as meningococcal meningitis. The infection causes inflammation of the meninges or membranes surrounding the brain and spinal cord, leading to pyogenic abscess (Figure 4). The infection can spread via respiratory droplets of an infected human host. In fact, Meningococcal species can only infect humans and have never been isolated from animals because the bacterium cannot get iron other than from human sources (transferrin and lactoferrin).
Figure 4. Neisseria meningitidis in spinal fluid. Click to enlarge. This pathogen is able to cross the mucosal barrier and enter
the bloodstream. However, how the infection
spreads the central nervous system is not fully
understood.
Systemic infection only occurs in those lacking
serum bacterial antibodies
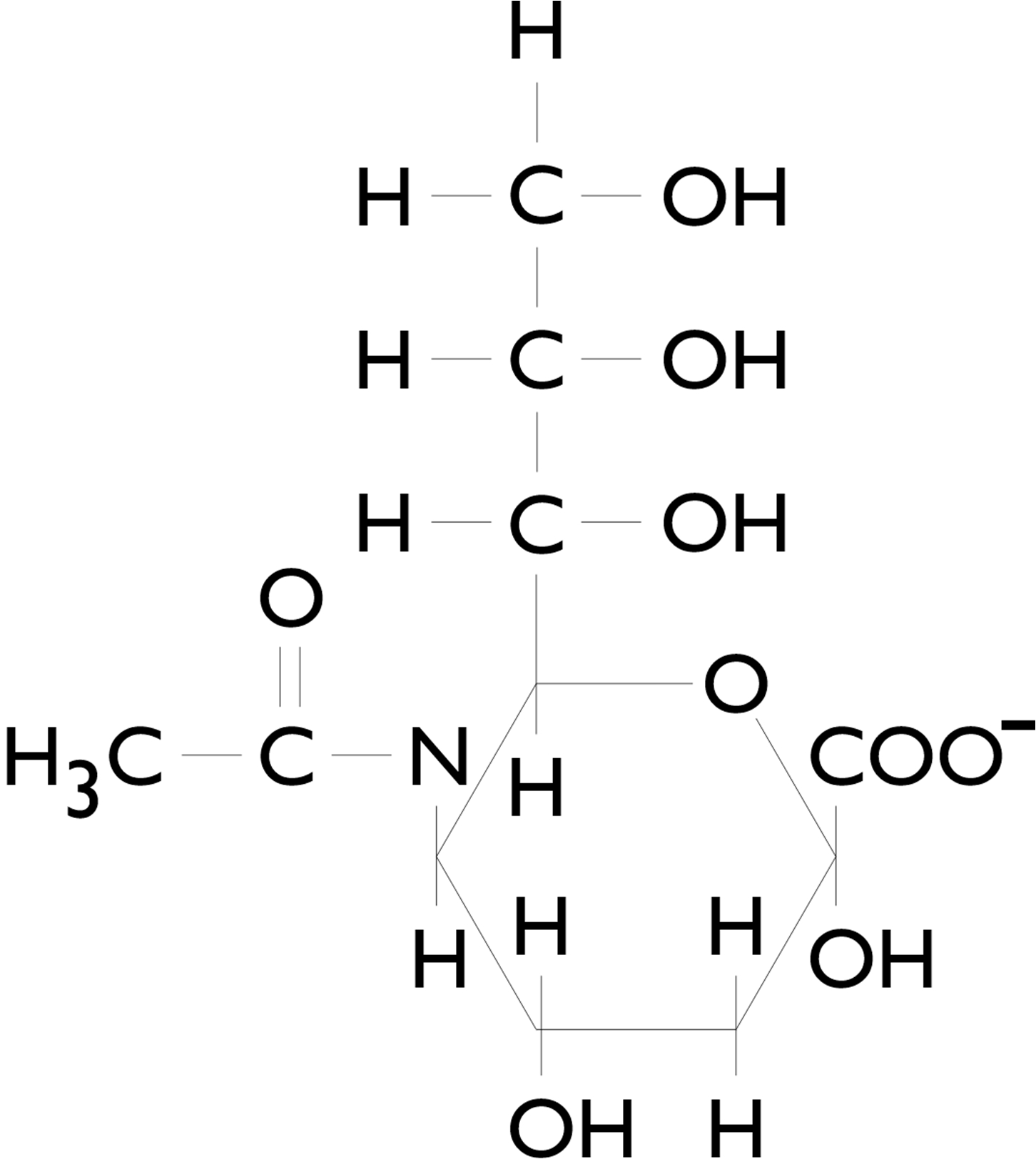
specific for antigens of this strain, or those
that lack late-acting complement Figure 5. Chemical structure of sialic acid. There are a number of host defense mechanisms to prevent meningitis from occurring. The pharyngeal and respiratory epithelium acts as a physical barrier. Irritation or damage of the mucosa may cause upper respiratory infection, and may lead to invasive disease. Serum bactericidal Immunoglobulin G (IgG) and immunoglobulin M (IgM) are the most important host factors. These antibodies are produced because other Neisseria species are part of the microflora of the upper respiratory tract. Common symptoms of the infection include fever, chills, headache, lack of appetite, vomiting, and dehydration. More serious neurological conditions include apnea, seizures, motor disturbance, coma, spinal rigidity, hamstring spasms, and exaggerated reflexes. Physical signs of the infection include petechiae (hemorrhagic spots in the skin) or purpura (multiple small hemorrhages into the skin). However, purponic rashes are mainly associated with septicaemia caused by N. meningitidis, a disease that receives much less public attention than meningococcal meningitis, even though it has been linked to infant deaths. Treatment and Prevention: The disease is curable with the help of antibiotics. Penicillin treats meningitis by penetrating the blood-brain barrier when the meninges are inflamed. Chloramphenicol or cephalosporin is used when the patient is allergic to penicillin. People in close contact with infected individuals require chemoprophylactic agents such as rifampin to protect them from contracting meningococcal disease. Vaccines are available for groups A, C, AC, and ACYW135 capsular polysaccharides. These vaccines are not very effective in children under the age of four. A universal vaccine is not currently available as there is variation of proteins on the surface of the bacterium. Also, natural selection results in new antigenic variants due to the continued exposure of the bacteria to different host. An outer membrane protein, PorA, has been a target for a vaccine-induced antibody; however, different strains have different amino acid sequences within the binding region, making it difficult to find a universal antibody. PorA has some amino acid loops that are potential targets for antibodies. The disease caused by N. meningitidis can be life-threatening if left untreated; however, with proper treatment, an individual can usually make full recovery without many lingering side effects. References: DeVoe, I. W., & Gilchrist, J. E. (1978). Piliation and colonial Morphology Among Laboratory strains of Meningococci. Journal of Clinical Microbiology , 379-384. Singleton, T.E., Massari, P., Wetzler, L.M. (2005). Neisserial Porin-Induced Dendritic Cell Activation Is MyD88 and TLR2 Dependent. Journal of Immunology, 174: 3545-3550. |
Diplococcal: A diplococcus (plural diplococci) is a round bacterium (a coccus) that typically occurs in pairs of two joined cells (shown below).

|