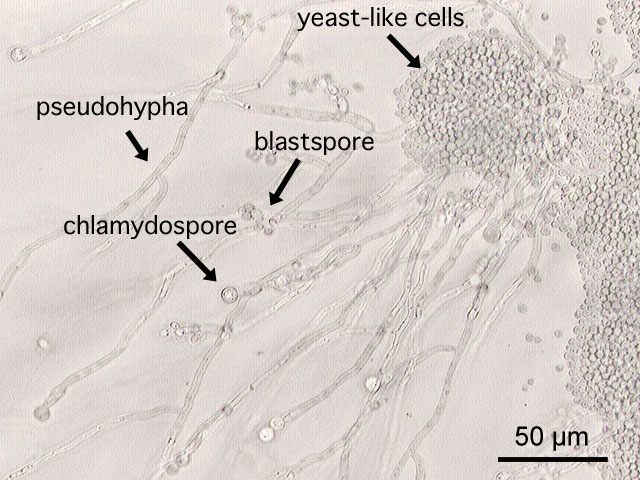
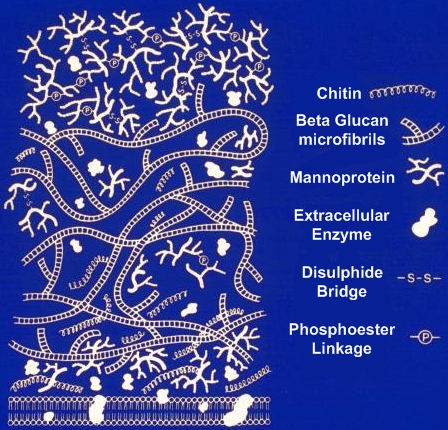
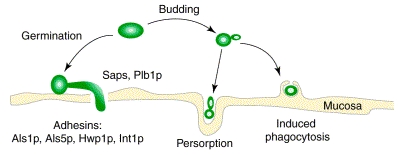
Candida albicansOverview: Candida albicans is a unicellular, oval-shaped diploid fungus (a form of yeast) that lives on various mucosal surfaces of the body, including the oral cavity, gastrointestinal tract, and vaginal mucosa. The organism is dimorphic and changes from one morphological form to the next in different environmental conditions. Most yeasts do not produce mycelia, but this is not the case for C. albicans. Normal room temperatures or even anaerobic conditions favour the yeast form of the organism, which reproduce by budding and are typically 10 to 12 µm (micrometres) in diameter, but under physiological conditions (body temperature, pH, and the presence of serum) it may develop into a hyphal form called pseudohyphae. The formation of pseudohyphae occurs by polarized cell division when yeast cells growing by budding have elongated without detaching from adjacent cells; thus, the cells remain attached to each other. Chlamydospores may also be formed on the pseudomycelium; these structures are round, refractile spores with a thick cell wall (Figure 1). The transition from a commensal to a pathogenic lifestyle involves changes in environmental conditions and dispersion within the human host. In fact, an overgrowth of the invasive, multicellular filamentous pseudohyphae form results in the fungal infection candidiasis or thrush. Figure 1. Various morphological forms of Candida albicans. Although the terms dimorphism and dimorphic fungus, meaning the species exists in two morphological forms, are well established and commonly accepted when referring to C. albicans, strictly speaking this fungus has the ability to adopt a spectrum of morphologies, and thus C. albicans could be considered a polymorphic or pleomorphic organism. Some strains of C. albicans are known to undergo phenotypic switching, a process in which different cellular morphologies are generated spontaneously. One of the classically studied strains that undergoes phenotypic switching is WO-1, which consists of two phases, namely, one that grows as round cells in smooth white colonies and one that is rod-like and grows as flat gray colonies. The other strain known to undergo switching is 3153A; this strain produces at least seven different colony morphologies. In both the WO-1 and 3153A strains, the different phases convert spontaneously to the other(s) at a low frequency. The switching is reversible, and colony type can be inherited from one generation to another. Approximately 80 to 90% of the cell wall of C. albicans is carbohydrate. Three basic constituents represent the major polysaccharides of the cell wall, namely, (1) branched polymers of glucose containing b-1,3 and b-1,6 linkages (b-glucans); (2) unbranched polymers of N-acetyl-D-glucosamine containing b-1,4 bonds (chitin); and (3) polymers of mannose (mannan) covalently associated with proteins (glyco[manno]- proteins). In addition, cell walls contain proteins (6 to 25%) and minor amounts of lipid (1 to 7%) (Figure 2). Figure 2. This illustration depicts the molecular architecture of the cell wall of a Candida albicans fungal organism. Virulence and Pathogenicity: C. albicans has several virulence factors which make it harmful to its host; one of which is its use of cell wall adhesins. Adhesin proteins promote the binding of the organism to host cells via hydrophobic interactions. This reduces the level of yeast clearance from the body under normal immune regulation (Figure 3). When C. albicans penetrates host mucosal surfaces following morphogenesis into invasive filaments, the polymorphic growing pattern helps the yeast invade host tissue by secreting various degradative enzymes, including various proteinases, aspartyl proteases, and phospholipases. Lastly, phenotypic switching also plays a role in altering the yeast's adherence properties, antigen expression, and tissue affinity. Switching might provide cells with a flexibility that results in the adaptation of the organism to the hostile conditions imposed not only by the host but also by the physician treating the infection. Figure 3. Early events in the pathogenesis of candidiasis are portrayed on a mucosal surface. A yeast cell of Candida albicans is shown either budding (right) or germinating (left). At the mucosal surface, germination of yeast cells (left) and penetration of the mucosa is shown. However, persorption of yeast cells (center) also results in the uptake of budding cells into the submucosa. On the far right, induced phagocytosis of a yeast by a mucosal cell is shown. These events are promoted by adhesins and enzymes. The germ tube is pictured as expressing different antigens compared with the yeast cell. The contribution of phenotypic switching to pathogenesis could be in promoting tissue-specific affinities for the organism as well as antigenic changes (Calderone & Fonzi, 2001). Clinical Infections: Since C. albicans is part of the normal flora, suggesting that it is normal for all humans to have controlled quantities of the organism. However, when a host is immunocompromised (people with AIDS, leukemia or cancer), C. albicans becomes an opportunistic pathogen, growing excessively and causing candidiasis. This is one of the reasons why doctors maintain that it important for females to eat healthy, because if not, the immune system can become suppressed and a yeast infection (vaginitis) can occur. Often, when a multitude of drugs are being taken to treat a particular infection, for instance, those with stomach ulcers taking a cocktail of antibiotics, bacteria that are part of the normal flora that keep C. albicans growth in check are killed. This gives C. albicans the opportunity to proliferate (Calderone and Fonzi, 2001). Infections caused by this pathogen normally occur at the mouth, skin or vagina. It is also possible for C. albicans to infect the penis, though this more common in uncircumcised men who have had sexual intercourse with an infected partner. When there is infection of the mouth, it is known as thrush. White and creamy blue patches are visible on the tongue and walls of the mouth when thrush occurs. This is typically accompanied by an inflamed tongue that is more red in colour (Figure 4). The person may experience a loss in taste sensation or may wake up with a sour mouth. When in the vagina, the infection is known as vaginitis or yeast infection. This is characterized by a white or yellow discharge, as well as burning, itching, and inflammation of the vagina and vulva. C. albicans can cause candidal onchomychosis in the nails or the area around the nail. The infection appears red and swollen, is often painful and pus can develop after some time. Figure 4. Thrush caused by Candida albicans. When a person is severely immunocompromised C. albicans may be able to enter the bloodstream. An infection of the bloodstream can causes serious problems, especially in the kidneys, heart, lungs, eyes, brain, and many other organs. Symptoms of this systemic spread are commonly fever, chills, anemia, rash and shock, but other symptoms can be apparent depending on the organ affected. The role of T helper 1 (TH1) and T helper 2 (TH2) cytokines play a key role in infection. Treatment of mice with blocking antibody against interferon-γ (TH1 cytokine) leads to progressive infection with C. albicans in mice that were previously immune. In addition, mice treated with antibody to IL-4 (TH2 cytokine) recover from an otherwise lethal inoculum of C. albicans. Treatment: In clinical settings, candidiasis is commonly treated with antimycotics. The antifungal drugs commonly used to treat candidiasis are topical clotrimazole, topical nystatin, fluconazole, and topical ketoconazole. For example, a one-time dose of fluconazole (as Diflucan 150 mg tablet taken orally) has been reported as being 90% effective in treating a vaginal yeast infection. This dose is only effective for vaginal yeast infections, and other types of yeast infections may require different treatments. In severe infections (generally in hospitalized patients), amphotericin B, caspofungin, or voriconazole may be used. Local treatment may include vaginal suppositories or medicated douches. Gentian violet can be used for breastfeeding thrush, but when used in large quantities it can cause mouth and throat ulcerations in nursing babies, and has been linked to mouth cancer in humans and to cancer in the digestive tract of other animals. C. albicans can develop resistance to antimycotic drugs, such as fluconazole, one of the drugs that is often used to treat candidiasis. Recurring infections may be treatable with other anti-fungal drugs, but resistance to these alternative agents may also develop. References: Calderone, R.A., and Fonzi, W.A. (2001).Virulence factors of Candida albicans. Trends in Microbiology, 9(7): 327-335. |